YouTube Links to Hip Range of Motion Exercises and Anatomy Lessons of the Hip, Thigh, and Knee. These Muscles Affect Your Entire Body Including the Pelvic Floor, the Neck, and Even the TMJ
- Tara Lee Clasen

- Mar 9
- 26 min read
Updated: Apr 2

The movement of your feet, legs, and hips influences everything in your body. This blog post is for those wanting to educate themselves on which muscles control femur movement. In this blog post, you will find YouTube videos that explore the motion of the femur as it sits in the hip socket and the lower leg. I have another blog post that defines all the muscles of the lower leg—the muscles that cover the tibia and fibula—and in that post; I share YouTube videos that affect the ankle. You can find that post HERE
When we talk about hip movement, we are talking about the dynamic movement of the femur as it sits inside the pelvis. Hip motions are flexion, extension, rotation, abduction, and adduction of the thigh (the femur). The movement of the femur moves the pelvis. You can see this during the gait cycle (the walking cycle). When you move a leg backward (extend it), the pelvis moves backward on the same side. The pelvis and the sacrum have their own motions. The pelvis tilts and rotates. Muscles that originate on the pelvis attach to the thigh and affect hip movement (femur movement). Hip motion is what this post focuses on, but in the muscle descriptions, you might see the mention of the pelvis, as these muscles are all stabilizing the pelvis.
As pelvic stabilizers, the hip muscles affect the pelvic floor. The pelvic floor affects the jaw. When you walk, your feet should be neutral in their pronation, as overpronation affects the knees, the hips, and the entire structure upwards. As a jaw, neck, and pelvic floor therapist, I understand the importance of whole-body health. The women-focused therapy I offer is hands-on and direct to the TMJ and cervical spine, and the muscles inside the pelvic bowl. This hands-on work ends migraines, headaches, throat constriction, TMJ clicking, TMJ pain, ear pain, ear fullness, bladder leakage, bladder pain, and chronic pain of the jaw, TMJ, neck, and pelvic floor. To assit with breathing, I also work on the diaphragm and psoas.
I only see women who reach out for pain and dysfunction in those areas mentioned: the jaw, the TMJ, the neck, the diaphragm, and the pelvic floor. Whereas the intravaginal pelvic floor work can branch out to other necessary areas, I do not see women for pain in the feet or lower limb dysfunction. I enjoy referring women to other practitioners to keep my working hours free for jaw, TMJ, neck, and pelvic floor therapy. These blog posts about the feet and legs are to serve as resources for the women I see with those other complaints.
What You Will Find in This Post...
Soft Tissue Connection (my thoughts in whole body health)
What the Hip Influences
Links to Other Blog Posts
YouTube Video Links
Defining Hip Movements
The Muscles of:
Iliacus or Iliopsoas
Psoas
Psoas Minor
The Quadriceps
* Rectus Femoris
* Vastus Lateralis
* Vastus Medialis
* Vastus Intermedius
Articularis genus
TFL
The Adductors
* Adductor Longus
* Abductor Brevis
* Adductor Magnus
Sartorius
Semimembranosus
Semitendinosus
Bicep Femoris
Popliteus
Popliteus Fossa
This post also contains information on quadricep tendonitis and the pes anersinus and pes anserine bursitis and pes anserine tendinitis .
A quick reminder that inflammation is under the influence of the gut! This is one of my favorite gut products. Use the code TLC at checkout and save 15%.
Click the pictures to head right to each product (but use TLC at checkout for the discount):

Soft Tissue Connection
The femur is the longest bone in the body, and how it moves affects the pelvis, and how the pelvis moves affects the spine. Please note that there are joints and joint dysfunction, and there is soft tissue—muscles, nerves, and myofascial tissue—and soft tissue dysfunction. Over time, soft tissue dysfunction affects joints. You can have soft tissue dysfunction in your pelvis, but imaging will show your pelvic and related bones and joints looking fine. The pull, hypertension, weakness, and overall dysfunction of your soft tissue will be what is causing you pain and what will later cause your joint problems.
This article is focusing on hip movement and teaching you to notice how you move. But I also want to encourage you to notice how you feel and think of your structure as one whole being. You have muscles, which the article defines below, and these muscles touch each other and touch nerves, myofascial tissue, and organs, and all of that works together. Continuous layers of myofascial tissue cover those muscles and share information through that tissue. I just want to point that out so as you read, you hold space for the influences of more than bone and joint motion.
What the Hip Influences
The movement of the femurs in the hip joints, which is called hip movement, affects the pelvis. Having healthy hip muscles and hip movement aids the body in maintaining a neutral and stable pelvis, which affects the lower back.
The angle of the femur in relation to the knee (femoral torsion) can either stabilize the feet and the pelvis, or can lead to compensatory patterns. As an example, if the pelvis were to tilt slightly forward, your hip flexors, pelvic floor, and abdominals would be affected. A disrupted core would then create other types of rib cage and spine dysfunction.
If in combination with other correlating conditions—sitting in an office chair, leaning forward when lifting weights, or running with a disrupted stride—the pelvic tilt would increase, and the low back would cope by developing “hyperlordosis,” a condition where the low back curve increases. This can lead to soft tissue pain and, eventually, arthritis.
To learn about the muscles of the lower leg and see the "ankle exercise"YouTube videos that I recommend, head "Does One Foot or Both Feet Rotate Out When Walking? Duck Feet? This Can Stem From An Imbalance in the Femur (the Hip), Tibia (Lower Leg), or the Ankle and Foot. Find Details Here" HERE
To learn more about anterior pelvic tilt, head HERE (COMING SOON!)
To learn about how the hips affect the pelvic floor, head HERE (COMING SOON!)
To learn about why your feet may be externally rotated, head HERE (COMING SOON!)

YouTube Video Links
I admit at the time of writing this, that I have not really watched these videos in their entirety. But I gathered enough quick info to know this is a nice collection for those who want to learn more. These videos would also help you understand my blog post about external foot rotation.
Simple Video on Externally Rotated Feet
Pronation glut strength fix:
More explanation as to reasons for external rotation:
Zac Cupples P.T Explanation on Some Reasons for External Rotation
Conner Harris (Personal Trainer) Hip and Pelvis Rotation and Walking
Tom Morrison How to Improve your Internal Hip Rotation
Precision Movement Explains Pronation and External Rotation (and More!)
Video on Knee Valgus and Exercise
Tibia External Rotation Exercise
Pronation Glut Strength
Zac Supples PT Fix External Rotation
Dorsifelxion Foot Motion
Defining Hip Movements
***IMPORTANT*** When we talk about the movement of the femur as it rotates in the hip socket, we call it hip movement. This is different from pelvic movement. When talking about moving the femur, or hip movement, the word “thigh” is also often used. A muscle that internally rotates the femur can also be described as moving the thigh or hip. Pelvic stabilization and pelvic movement are affected by these same muscles, but the word pelvic or pelvis is used when describing its movement.
The ball and socket joint of the hip is extremely dynamic. The muscles that perform the actions are highlighted in pink.
The movements of the hip:
Flexes
Hip flexion is when the thigh comes closer to the torso. This happens when you raise a relatively straight leg or bend at the knee. Major muscles involved in hip flexion are: iliopsoas, rectus femoris, and psoas major.
Extension
Hip extension is the movement of the leg behind the body. It increases the angle between the femur and the pelvis. Major muscles involved in hip extension are: gluteal muscles and hamstrings.
Adduction
Adduction is adding your leg to your body. Adduction is the movement of bringing the leg toward the midline. Hip adduction involves the hip adductor muscles: adductor longus, adductor brevis, adductor magnus, gracilis, and pectineus.
Abduction
Abduction is taking your leg away from your body. Abduction is the movement of the femur away from the midline. The major muscles involved in hip abduction are: gluteus medius, gluteus minimus, and tensor fasciae latae.
Internal Rotation
When the head of the femur spins inwards, towards the midline, the femur internally rotates. The main muscles that turn the femurs inward are: tensor fasciae latae (TFL), gluteus minimus, and the anterior fibers of the gluteus medius.
External Rotation
When the head of the femur spins outward, away from the midline, the femur externally rotates. The main muscles that turn the femur outward are piriformis, gemellus superior, gemellus inferior, obturator internus, obturator externus, quadratus femoris.
Muscles of the Upper Leg

Iliacus or Iliopsoas
The iliacus and psoas work together to flex the hip, and their connection is so close that people often call the iliacus the iliopsoas. Iliacus, in the photo above, is the muscle hugging the inside of the pelvic bone. This muscle can cause a lot of problems that may seem unrelated to the local area, and although many struggle with pain or dysfunction here for years, it is possible to heal. Look for a skilled soft tissue manual therapist who will patiently spend time therapeutically working on this area. It is also possible to learn to release it yourself with a tool you can find HERE (Scroll to find Generic Hip Hook). Even if you can work on it yourself, I would still highly recommend finding a soft tissue provider to assist you. You may need to "shop around" to find a soft-tissue therapist who can really work on this area. Some soft tissue therapists may even work on the upper part of the psoas but struggle to work inside the crest of the pelvis.
The iliacus arises from the iliac crest, the iliac fossa, the lateral aspect of the sacrum, and the anterior sacroiliac and iliolumbar ligaments. The iliacus then blends with the tendon of the psoas and inserts onto the femur.
This muscle produces thigh flexion. It will also move the torso forward.
When the pelvis is still, it flexes the thigh (hip). When the femur remains stationary, it will bring the torso into flexion against resistance. These actions are aiding you when running, walking, and jumping.

Psoas
The psoas is a major hip flexor and, as mentioned when defining iliacus above; it shares a common tendon with iliacus. Having a healthy and happy psoas is very important. When the psoas is tight, it will cause pain in the front and/or back of the body. It can cause an anterior pelvic tilt, which alters the ribcage and spine. I often work the psoas during TMJ-focused sessions. This muscle has a relationship with the jaw muscles. On some people, they feel the jaw when we work this muscle and when we work certain muscles in the jaw, they will feel this muscle.
Posas has various roles in hip movement. Information on psoas movement can vary because researchers did not perform some original movement studies on adult subjects. In a recent study that focused on adult anatomy, when in normal anatomical position, the psoas acted as a hip flexor with little rotational component.
With the hip already at 90 degrees of flexion, when the psoas is further engaged or tractioned, there will be slight adduction.
When the hip is already in abduction, moved away from the body, the psoas assisted with up to 30 degrees of lateral/external rotation. With the hip already in an adducted position, close to the body, the psoas played no role in rotation. It is possible that other studies could contradict these findings; however, one could take from this information that the psoas is not a major player in rotational issues. That said, many people have tight hip flexors, and so you could address the psoas for this reason. And I believe, an excessive internal rotation could create a pinch and pain in the hip flexors.
Psoas Minor
Researchers roughly estimate that 40-65 percent of the population has a psoas minor that lies on top of the psoas, or psoas major. People can miss this muscle or have variations of it with no known consequences.

The Quadriceps
The quadriceps femoris is the strongest muscle(s) in the body. Latin defined quadriceps femoris as “four-headed muscle of the femur.” The quadriceps femoris comprises the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius.
As a group, not only act upon the hip but they also act upon the lower leg. Below, each quadriceps will be mentioned. But if you read the post on external rotation (again HERE--COMING SOON), you might be craving :) to know more details about how the quadriceps move the tibia. Below is a brief explanation.
How quadriceps move the tibia:
The quadriceps connect to the patella, and the patellar tendon connects the patella to the tibial tuberosity on the front of the tibia. When the quadriceps contract, they transmit force to the tibia via the patellar tendon, and the tibia shears forward and upward. This extends the lower leg; the leg straightens.
As the lower leg straightens, the tibia externally rotates. Knee extension, straightening the leg, biases the tibia towards external rotation, while flexing the knee, bending the knee, biases the knee towards internal rotation.
Thinking about these motions in relation to when you experience pain or to your limited range of motion can help you determine what is happening to your tibia.
But it also shows us that since the quadriceps transmit a force that ultimately externally rotates the tibia (upon extension), overly hypertonic—tight and tense and inflamed quadriceps muscles—may bring the tibia into excess external rotation, limiting internal rotation.
Below is each quadriceps muscle. As a group, these muscles are called quadriceps femoris and share a common tendon. As a group, these muscles are known for extending the hip. The quadriceps muscles form the anterior compartment of the leg with sartorius and and articularis genus.
The quadriceps muscles originate from locations on the femur, except for the rectus femoris, which arises from the iliac spine of the hip.

Rectus Femoris
Rectus femoris is a bulky muscle that runs straight down the leg (rectus means straight in latin) and assits the iliposas in flexion. It also works with the other quadriceps to extend knee. This muscle crosses two joints, the hip and the knee, unlike the next muscle, vastus lateralis, which only crosses the knee.
Rectus femoris pain can appear at its tendon which is on the spine of the pelvis. When it is tight, it will pull on the patella and through that, pull on the tibia bone. If you have developed a chronically tight rectus femoris on one side, the patella may appear higher on that side.

Vastus Lateralis
Vastus Lateralis is a deep muscle that runs down the lateral side of the leg. This is the largest of the quadriceps muscles. It extends the knee and stabilizes the knee. It affects the tbia through its connection to the patella, but after inserting onto the patella, part of its tendon actually continues to the head of the tibia. The illustration above does not show that, as it only shows its connection to the patella.
The vastus lateralis stabilizes the knee by creating a lateral pull that works against the medial pull of the vastus medialis. In patellofemoral pain syndrome, the vastus lateralis will contract prematurely causing the patella to become unstable and track laterally.
Sometimes people mistake vastus lateralis pain with dysfunction in their IT band. The IT band is a powerful and dense piece of myofascial tissue and does not change in the way people think it does. When you are foam rolling, you are affecting the brain, and you are affecting the vastus lateralis, and the connections between myofascial tissue and neuromuscular tissue.
I would hypothesize that in many of the cases where that reduces pain, it was likely the vastus laterals that was finding relief. Relief in this muscle and better function of the IT band can even come from creating a separation between these structures. The gliding movement of foam rolling takes a glue-like area and changes it to an area of lubrication.

Vastus Medialis
You may hear of the vastus medialis and you might hear of the VMO—the vastus medialis oblique. Sometimes people use those names interchangeably, causing confusion. The vastus medialis, on the inside of the leg, is the most medial quadriceps muscle. It runs from the top of the femur to the patella and the tibial tuberosity. The VMO is the last tear-shaped part of that muscle; the fibers change and run obliquely towards the knee.
The main part of the muscle extends the knee. The VMO acts medially upon the patella and assists during the end stage of knee extension. You need a healthy relationship between the lateral and medial quadriceps to stabilize the patella during flexion and extension.
About 15 years ago, the VMO was the catch-all explanation for any type of knee pain, and that drove me crazy. Weakness in the VMO can cause knee pain, as it will not balance the lateral pull of the quadriceps lateralis. The VMO is naturally a “bulky” part of the muscle, and the fiber orientation is unique. You can hypothesize that it is important to the body that the VMO be strong. People with pain because of patellofemoral pain syndrome will benefit from strengthening the VMO. There are studies that show how a weak VMO will cause patellar displacement during different phases of knee flexion. Remember that muscles produce their movements, and muscles act as agonists to the movements of other muscles, and this “push and pull” creates healthy joint tissue.
Vastus Intermedius
The fibers of vastus intermedius look like a feather, running obliquely from a central tendon. The tendon originates from the front of the femur, lateral to the midline. It has a close relationship with all quadriceps, touching the other three, but it appears inseparable from the vastus medialis (a thin line separates them until the tendon insertion near the femur head). It is the deepest quadriceps muscle and lies behind the rectus femoris, which is the most superficial.
It assists in knee flexion and has a connection to the patella and tibia.

Quadriceps Tendonitis
All the quadriceps muscles merge into a central tendon. The quadriceps tendon inserts onto the top of the patella. Although it is one continuous tendon, as the quadriceps tendon extends below the patella, it is called the patellar tendon. The patellar tendon is interesting as it connects bone to bone, the patella to the tibia, and therefore is sometimes called the patellar ligament (ligaments connect bone to bone). The medial and lateral aspects of the quadriceps tendon pass down the sides of the patella to merge onto the tibia. The superficial fibers run continuously over the patella to merge onto the tibia.
If you have pain above the kneecap (the patella), you have quadriceps tendinitis. If you have pain below the kneecap, you have patella tendinitis.
People commonly describe quadriceps and patella tendonitis as an “overuse” injury. One should describe it as a functional injury. If under load, the tendon repeatedly moves in a dysfunctional way, microtears and inflammation can result. You can injure the tendon and develop inflammation from a single event, but it also develops slowly.
If you exercise with a weak VMO and a hypertonic (overly contracted, tight) vastus lateralis, you place the tendon under an unhealthy force.
The body may have trouble clearing inflammation because of issues with the immune system. And so the causes of quadriceps and patella tendinitis can be multi-causal.
We can observe that the attached tissues influence the patella tendon, the quadriceps tendon, and the large and powerful quadriceps muscles.
But if you look at where the patella tendon connects on the tibia, and you think about the rotation of the tibia, you can see how the health and function of the shin bones will directly affect the patella tendon. The quadriceps muscles influence tibia position through the patella tendon, but as you learn about in a blog HERE (COMING SOON), the tibia is also under other forces. External rotation of the tibia is a risk factor for patella tendinitis. Ligament laxity is also a risk factor as that leads to lateral (external) displacement of the tibia.
Articlaris Genus
Articularis genus is a small little known muscle on the front of the tight by the patella (the knee). It is on the lower front of the femoral shaft deep to vastus intermedius, It inserts onto the suprapatellar bursa of the knee joint. Some sources consider this the fifth head of the quadriceps. The quads are the strongest and largest muscles, but this tiny muscle is close to them, lying deep to the vastus intermedius, and acting with them to support the knee.
Although small, the articlaris genus muscle is important in knee flexion and extension. When the knee is extended, the articlaris genus pulls the suprapatellar bursa upward. This keeps it safe from being caught between the femur and the tibia. Suprapatellar bursitis can be the result of dysfunction of this muscle.
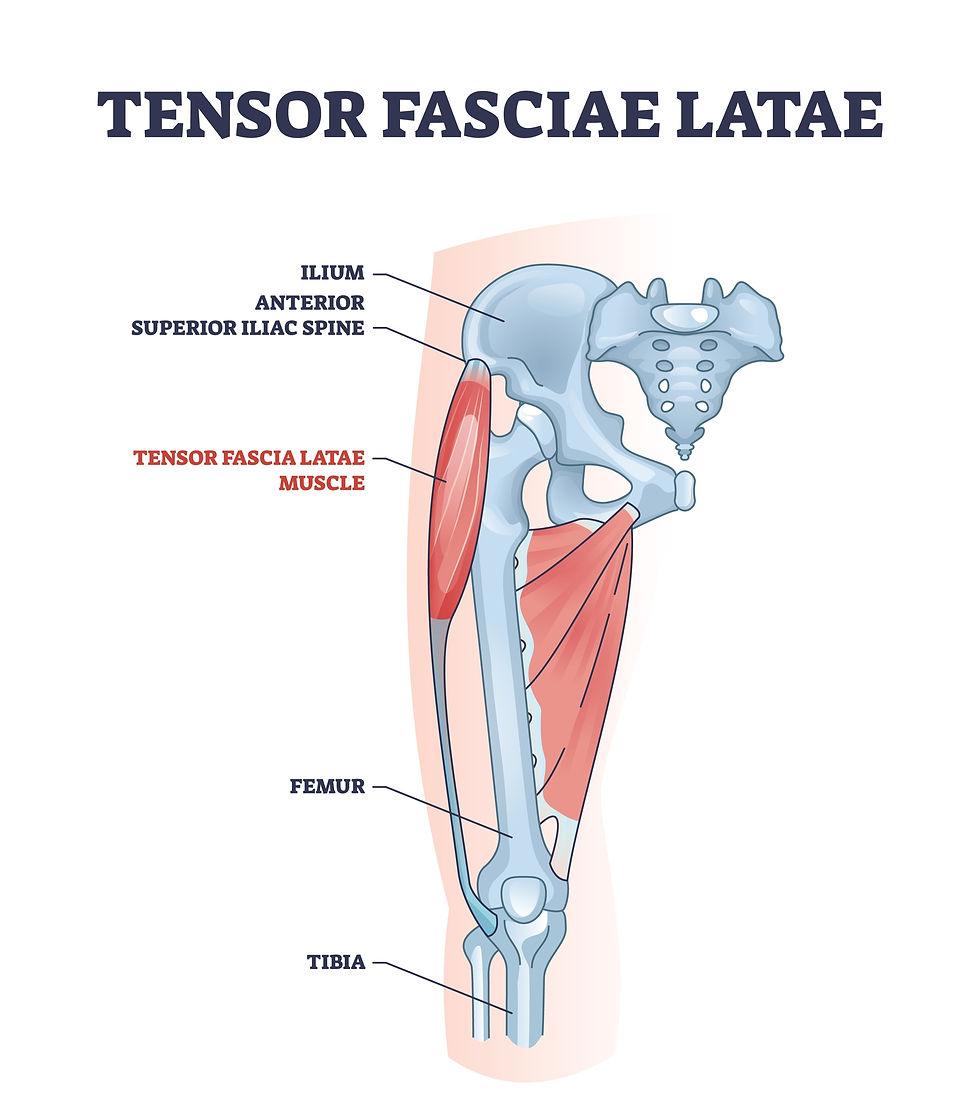
TFL
TFL pain can feel like referred pain down the side of the leg. It can feel diffuse, or vague, and even like you have some pain in your upper quad. TFL pain can also feel intense in the muscle's belly, there can be friction between it and bone, and it can also mix and blend with pain in the glutes.
TFL can be an issue for runners and soccer players, and for those who sit at a desk. A shortened (tight and tense) TFL can lead to an anterior pelvic tilt. Read more about that HERE (COMING SOON).
During standing and walking, the TFL is stabilizing the pelvis and one of TFL's main actions is to create tension on the IT band. TFL gives feedback to the IT band and works with the IT band to create stability and movement. Along with the IT band, it tenses and stabilizes the knee when the leg is extended.
A tight TFL will pull on the IT band and create excessive external rotation of the lower leg at the knee joint. As the knee flexes, the TFL acts upon the knee and a healthy TFL helps the knee track straight.
TFL is an accessory knee flexor, meaning it is not its major action, but it contributes to it. TFL mainly assists in knee flexion once someone has already lifted the knee to 30 degrees. The TFL assists in walking by pulling down on the ipsilateral hip (the same side) causing the contralateral (the opposite side) hip to rise. The rise of the hip allows the leg to swing through.
The TFL internally rotates the hip and abducts the hip. TFL tension can create an internal rotation of the femur, which leads to foot overpronation. Read more about femur internal rotation HERE (COMING SOON).
It is working with the glute maximus, glute medius, and glute minimus to create hip motions of flexion, abduction, and internal rotation.
While the TFL has a direct impact on the femur, its influence on the tibia is indirect. The TFL plays a role in healthy external rotation of the tibia but tension can create excessive external rotation.

Gracilis
Gracilis is one of five muscles in the adductor group. Acting on the hip joint, the addductors move the leg closer to the body, as well as perform other actions. Gracilis is the only adductor muscle that acts upon two joints, the hip and the knee.
This muscle is often described as “sheet like.” It originates from the anterior body of the pubis, the inferior pubic ramus, ischial ramus and attaches to the medial surface of the tibia.
is attched to the coxal bone and to the tibia
This muscle will contract with each step and stabilize the thigh and hip. Adductor (which includes several muscles) tendon stress can present as pain high on the inner thigh near the pelvis. Repetitive inner thigh motions, such as what happens when you kick a soccer ball, can create adductor strain.
The most superficial muscle on the medial part of the thigh, gracilis has the important job of assisting the hamstring muscles in knee flexion. During the gait cycle, this happens during the swing stage. When the foot is fixed to the ground, during the gait cycle, gracilis laterally wraps the femur and pelvis around the tibia.
At the hip joint, it performs flexion and adduction.
At the knee, it produces leg flexion and internal rotation.
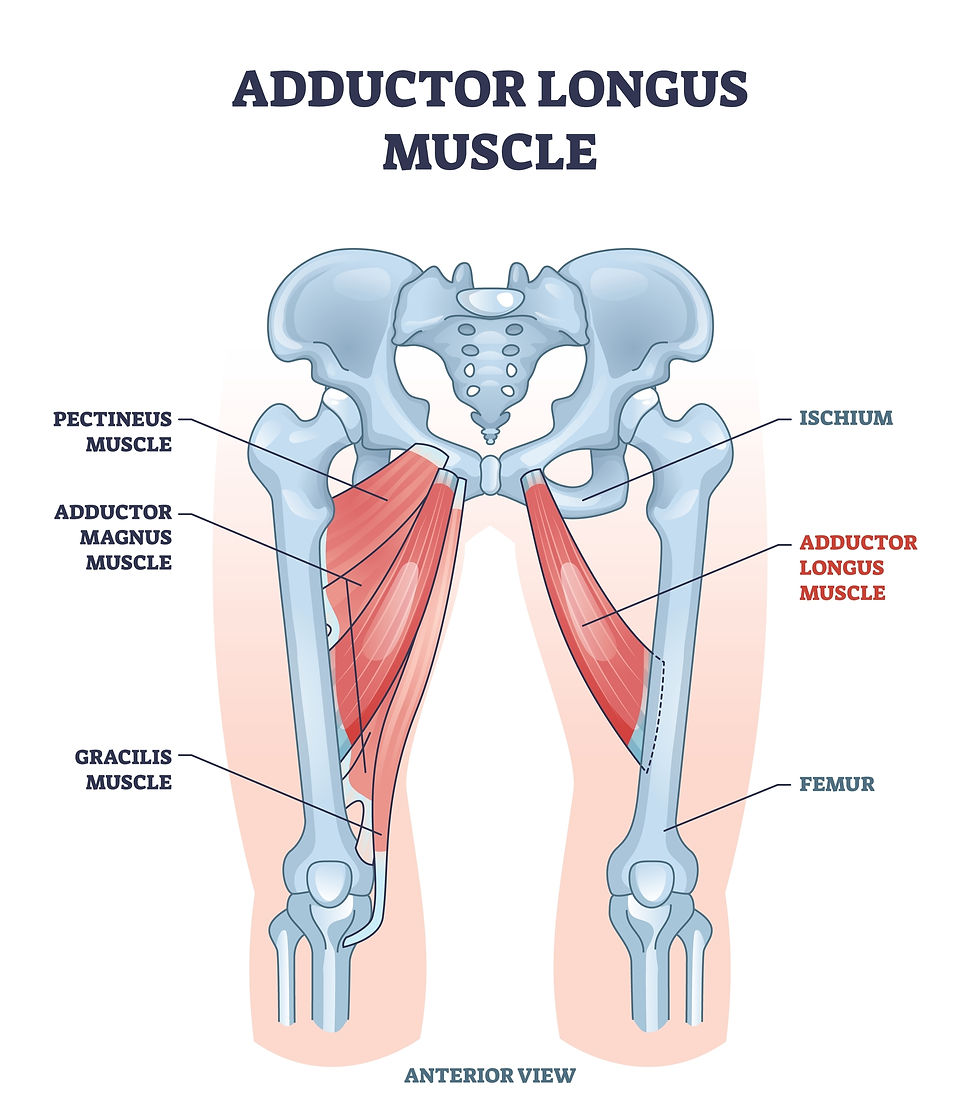
Adductor Longus
Adductor longus is one of five muscles in the adductor group. Acting on the hip joint, the adductors move the leg closer to the body, as well as perform other actions. Abductor longus is a large triangular muscle on the inside of the leg. It is one of the five muscles in the adductor group. In synergy with the other adductor muscles, it brings the femur closer to the body and stabilizes the pelvis. It is in front of the other adductors, magnus and brevis. Pectineus is lateral and gracilis is medial to its location. It originates from the body of the pubis, inferior to the pubic crest and lateral to the pubic symphysis. And it inserts on the middle third of the linea aspera of the femur.
It assists the hip flexors in flexing the thigh. With the other adductors, it adducts the thigh and externally rotates the thigh.

Adductor Brevis
Adductor brevis is a flat triangular muscle on the inside of the leg. It is one of the five muscles in the adductor group. In synergy with the other adductor muscles, it brings the femur closer to the body and stabilizes the pelvis.
Adductor brevis has a narrow origin on the anterior body of the pubis and the inferior pubic ramus and a large insertion which is on the linea aspera of the femur. This muscle lies deep to the adductor longus and pectineus and in front of the adductor magnus. The obturator nerve lies on its anterior and posterior sides.
At the hip joint, it produces hip flexion, thigh adduction, and external rotation.

Adductor Magnus
Adductor magnus is one of five muscles in the adductor group. Acting on the hip joint, the adductors move the leg closer to the body, as well as perform other actions. Adductor magnus is the largest adductor muscle. Though considered an adductor muscle, it also surprisingly includes a hamstring component.
It originates from the inferior pubic ramus and the ischial ramus of the pelvis and the ischial tuberosity. Adductor tension can cause sit bone pain, which is an important factor people rarely consider. It also inserts onto the gluteal tuberosity, linea aspera, and the medial supracondylar line, and the adductor tubercle of the femur.
Adductor pain can radiate into the lower abdomen.
The adductor part of the muscle engages the thigh in adduction and external rotation. The hamstring part aids in thigh extension and internal rotation. And the entire muscle works to stabilize the pelvis.

Pectineus
Pectineus is one of five muscles in the adductor group. Acting on the hip joint, the adductors move the leg closer to the body, as well as perform other actions. Pectineus is a flat muscle that is the most superior (above) adductor muscle.
With the adductor longus and the ilipsoas, it forms the femoral triangle. The femoral triangle is a passage where a major blood vessel pass from the pelvis and the lower limbs. Thick fascia covers the femoral triangle, separating it from the femoral artery.
Like all adductors, people can feel discomfort in the groin. Injury can be caused over time or by sudden overload. Overstretching with the legs out to the side or in front of the body can injure this muscle. If you look at the location of this muscle, you see that pain from a muscle strain will be near the pubic bone. Pain may radiate around the area and slightly downwards.
When it contracts, it first flexes the thigh, and then the fibers of the muscle work to adduct the leg. An example of a movement that uses both motions is crossing your legs. Being close to the pelvis, it acts as a important stabilzer of the pelvis.

Sartorius
Sartorius is the longest muscle in the body. It is thin and superficial with only skin and fascia over it. The large quadriceps muscles lie underneath, and the sartorius assists their actions. Sartorius crosses the knee and the hip. Starting at the corner of the ASIS (anterior spine of the iliac—the pelvis), its beautiful S-shape crosses the anterior surface of the leg, crossing medially and inserting at the proximal end of the tibia below the condyle.
Being a thin muscle, it does not produce strong actions, but it works with the other muscles to support their motions. At the hip, it aids in flexion, abduction, and external rotation. At the knee joint, it produces flexion and internal rotation. sartorius can both externally rotate the femur and internally rotate the tibia. Sitting cross-legged shows each of sartorius's actions.
Sartorius is interesting because of what it crosses over and touches: iliposaos, pectinueus, adductor longus, and TFL. It also blends its fibers with the medial collateral ligamant, the fibers of the knee joint, and the deep fascia. This aids in knee stabilization.

Pes Anserine
Pes anserine is the conjoined tendon of the sartorius, gracilis and semitendinosus on the tibia. Pes Anserine busitis is a inflammatory condition of the bursa that lies underneath this tendon and is a common cause of medial knee pain.
Pes anserine bursitis and pes anserine tendinitis usually occur over time and are sometimes called an “overuse injury.” The repeated motions of flexion and adduction create friction and pressure on the tendon and bursa.Tight hamstrings and lateral fitness motions can also create pressure on the bursa. But It is not just motion but rather dysfunctional motion from a disrupted soft tissue and possibly joint structure that creates inflammation and disease.
Pes anserine inflammation can be mistaken for or coincide with a stress-fracture, osteoarthritis, an MCL tear, and other.

Semimembranosus
Semimembranosus is one of the three hamstring muscles. Located on the posteromedial side of the thigh, and originating from the ischial tuberosity and complexly inserting onto six different locations.These 6-insertion locations are little known or talked about, but if you look at where they lie, the implications for how these insertions affect and communicate with the leg are tremendous.
Semimembranous inserts onto:
1) The posteromedial tibia
2) The medial collateral ligament.
3) Oblique popliteal ligament
4) An insertion directed towards the posterior oblique ligament, which is connected to the knee capsule.
5) Meniscotibial ligament (coronary ligament) of the posterior horn of the medial meniscus
6) Fascia that extends over the back of the knee and the popliteal fascia.
The main insertion of semimembranous is the medial condyle of the tiba, a prominent part of the tendon inserts onto the oblique popliteal tendon with some soruces (Ken Hub) stating it actually becomes part of the oblique popliteal tendon. That popliteal tendon insertion then connects to the posterolateral condyle of the femur.
Reports show variations in insertions and for some people, additional insertions. A bursa separates the semimebransous from the medial head of the tibia and the medial gastrocnemius.
At the hip joint, the it extends the and internally rotates the tight.
At the knee joint, it flexes and internally rotates the leg.
It stabilizes the pelvis
When the feet are on the ground, it extends the hip, which helps create an erect torso. When the hip is extended, the semimembranosus and semitendinosus internally rotate the thigh. Assisting with knee flexion and internal leg rotation occurs when the leg is off the ground.
When you are standing, the posterior thigh muscles are quiet. When you start to lean forward, these muscles activate to stabilize the hip and counteract the forward tilt.

Semitendinosus
Semitendinosus is the posterior muscle of the thigh, and one of the three muscles in the hamstring group. It shares its origin with the long head of the biceps femoris on the superior part of the ischial tuberosity.The attachment is deep to the gluteus maximus muscle. It travels inferomedial, and it blends with the fibers of gracilis and sartorius to become the Pes Anserine tendon and inserts on the proximal end of the tibia below the medial condyle.
It has a large, round tendon that comprises half of its mass. The function of the muscle depends on the starting position.
Generally, at the hip joint, it performs thigh extension, thigh internal rotation, and stabilizes the pelvis. At the knee joint, it performs leg flexion and internal rotation of the leg.
When in anatomical position, it internally rotates the thigh. If you flex your truck, semitendonosus extends the thigh. With a flexed knee, it internally rotates the leg. With the lower leg straight, it flexes the leg. With the knee is semi-flexed it assits semimembranous in internal rotation.
It stabilizes the pelvis and the knee.
When you are standing, the posterior thigh muscles are quiet. When you start to lean forward, these muscles activate to stabilize the hip and counteract the forward tilt.

Bicep Femoris
The bicpes femoris has two heads. That means there are two places of origin and that those tendons run together as they become the muscle’s belly. The long head originates inferomedial side of the ischial tuberosity and the sacrotuberous ligament The short head inserts on the lateral aspect of the linea aspera of the femur and the lateral supracondylar ridge of the femur. It inserts on the lateral aspect of the fibula.
The biceps femoris is the one hamstring muscle that aids in external rotation as opposed to internal rotation. It is on the lateral side of the back of the leg and has a lateral attachment site. Tension placed on the fibular head contributes to tibia external rotation. If you imagine a muscle pulling on the outer edge of the lower leg from behind, you can see how this would cause an external rotation. The pivot point (a joint that allows for rotation on a single axis) of the fibular head creates tension that—especially when there is knee flexion (during walking or strenuous and load-bearing activities)—will pull on the tibia.
The bicep femoris has the natural action of externally rotating the lower leg, but again, when tight, the external rotation motion will be excessive.
Biceps femoris acts on the knee and the hip. The complete actions of biceps femoris are thigh extension, thigh external rotation at the hip joint and at the knee joint, leg flexion, leg external rotation, and stabilizing the pelvis.
Biceps femoris hip extension action is strongest when bringing a bent forward trunk to a straight position. When the hip is extended, it assists in externally rotating the thigh.
When the leg is in anatomical position, a fixed position, flexion of the leg is its major action. When the knee is already semi-flexed, the biceps femoris externally rotates.

Popliteus
The popliteus muscle is unique as it is in the posterior compartment of the knee with the muscles of the lower leg, but unlike those muscles, its action is on the knee and not on the ankle. It is a deep muscle and forms part of the floor of the popliteal fossa.
The popliteus originates from the lateral condyle of the femur and the posterior horn of the lateral meniscus of the knee joint, and it inserts onto the posterior surface of the proximal tibia. The popliteus tendon is unique because it remains outside the knee’s synovial membrane, even though it’s enclosed within the knee capsule. It is a deep muscle
When the foot and lower leg are in a fixed position, the popliteus laterally rotates the femur as the knee flexes. During the gait cycle, when the foot contacts the ground, the tibia rotates laterally relative to the femur. This locks and stabilizes the knee. As the knee flexes, the popliteus contracts and rotates the femur laterally. This is the popliteus acting upon the femur and is the mechanism of unlocking the knee.
When the foot and lower leg are not fixed, the foot floats in the air. When this happens, the tibia and femur condyle surfaces align, and the knee becomes stable, allowing for smooth flexion and the controlled swing phase of the gait cycle.
ACL repair can damage the popliteus, which often tightens after the surgery. One study showed that undiagnosed popliteus injury leads to poor rehabilitation after knee surgery.
If the knee is locked in place, consider popliteus.

Popliteal Fossa
The popliteal fossa is a diamond-shaped depression at the back of the knee where the popliteal artery and vein, tibial and common fibular nerves, and lymph nodes pass through.
The popliteal fossa is formed superolateral by the biceps femoris muscle, superomedial by the semimembranosus and semitendinosus muscles, and inferiorly by the medial and lateral heads of the gastrocnemius muscle. The floor of the fossa is the deep popliteal muscle.
Resources are listed below.
Want to Know More?
I have more posts coming soon,. Stay tuned!
Check out my books on health and wellness!

The Elemental Woman
A Conversation for the Modern Western Woman Inspired by the Healing Wisdom of the Ancient Eastern Sage

Food & Mood Journal
A tracking guide to connect the food you eat, the emotions you feel, and increase the feeling of deep self-love

Mindful Movement Journal
A tracking guide to connect the motions you make, the emotions you feel, and increase the feeling of deep self-love
Basic Ayurveda
The Elemental Woman Supplement Guide
About the author:
Since 2004, Tara Lee Clasen has been assisting women on their healing adventures. As a woman-focused physical medicine provider, also trained in Eastern medicine, she knows transformation is possible and knows that with reflection and self-love, your future is full of bright possibilities.
#tmjpain #tmj #neckpain #shoulderpain #ribpain #chronicpain #jawpain #headaches #migraine #whiplash #asthma #vagusnerve #massagetherapy #manualtherapy #chiropratic #tmjpain #tmj #neckpain #shoulderpain #ribpain #chronicpain #jawpain #headaches #migraine #whiplash #asthma #vagusnerve #massagetherapy #manualtherapy #chiropractic #feet #Ankle #lowerleg #kneepain #ACL #ACLtear #meniscus #anklepain #dorsiflex #plantarflex #Anklemovement
Resources:
Miller, A, Heckert, KD, Davis, BA.The 3-Minute Musculoskeletal & Peripheral Nerve Exam. New York: Demos Medical Publishing. 2009; p.116-117
Page, P, Frank, CC, Lardner, R. Assessment And Treatment Of Muscle Imbalance: The Janda Approach. Sheridan Books, USA; 2010.
Peng YL, Tenan MS, Griffin L. Hip position and sex differences in motor unit firing patterns of the vastus medialis and vastus medialis oblique in healthy individuals. Journal of Applied Physiology. 2018 Jun 1;124(6):1438-46.
Castanov V, Hassan SA, Shakeri S, Vienneau M, Zabjek K, Richardson D, et al. Muscle architecture of vastus medialis obliquus and longus and its functional implications: a three-dimensional investigation. Clin Anat. 2019 May;32(4):515-523. doi:10.1002/ca.23344
Saladin. Anatomy & Physiology (7th ed.). McGraw Hill. p. 347.
Trammell AP, Nahian A, Pilson H. Anatomy, Bony Pelvis and Lower Limb, Tensor Fasciae Latae Muscle.Available: https://www.ncbi.nlm.nih.gov/books/NBK499870/ (accessed 27.12.2021)
BOOK:
Palastanga,. . Anatomy and human movement: structure and function (6th ed.).(2012)
Mochizuki T, Akita K, Muneta T, Sato T (2004). "Pes anserinus: layered supportive structure on the medial side of the knee". Clin Anat. 17 (1): 50–4. doi:10.1002/ca.10142. PMID 14695588.
Mohseni M, Mabrouk A, Li D, et al. Pes Anserine Bursitis. [Updated 2024 Jan 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532941/
De Maeseneer M, Shahabpour M, Lenchik L, Milants A, De Ridder F, De Mey J, Cattrysse E. Distal insertions of the semimembranosus tendon: MR imaging with anatomic correlation. Skeletal Radiol. 2014 Jun;43(6):781-91
Palastanga N, Field D, Soames R. Anatomy and human movement: structure and function. Elsevier Health Sciences; 2012.
Krudwig W K, Witzel U, Ullrich K 2002 Posterolateral aspect and stability of the knee joint Knee Surg., Sports Traumatol, Arthrose, 10:91-95.
Grob K, Gilbey H, Manestar M, Ackland T, Kuster MS. The anatomy of the articularis genus muscle and its relation to the extensor apparatus of the knee. JBJS Open Access. 2017 Dec 12;2(4). BibTeXEndNoteRefManRefWorks
Williams CH, Jamal Z, Sternard BT. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 24, 2022. Bursitis. [PubMed]
Psoas major and its controversial rotational action

Comments